By: Timothy Kays
With COVID-19 cases spiking over the last six weeks, an informational teleconference was facilitated by the Williams County Health Department on December 7 to disseminate the most current data on the pandemic in Northwest Ohio.
Attending the meeting via computer or phone were Williams County Health Commissioner Jim Watkins, Williams County Health Department Director of Education and Preparedness Victoria Smith, Chad Tinkel, the President/CEO of Community Hospitals and Wellness Centers (CHWC), Sally Taylor the Vice President of Parkview Physicians Group, and Dr. Kevin Park, Williams County Coroner and medical director at multiple area nursing homes.

Watkins gave a general overview of the current COVID status, saying, “Recently, I think that we’ve seen some encouraging signs with more people wearing masks in the community. We’re very happy that we had the formation of a group of residents and businesses that have all come together to set up our COVID defense team in the community to try and get us headed in the right direction, because this is going to take a lot of working as individuals in the community to keep residents safe.”
Ms. Smith referred to a slideshow presentation detailing the current numbers dealing with COVID in the county. “Williams County has reached level three or the red level,” she said, “…and has also triggered high incidence. This is our seventh week of reaching high incidence, which means 100 new cases per 100,000 residents in the past two weeks.”
“It’s also our fourth week, reaching level three or red. Across Ohio, many other counties share the same status as us, and several other counties have reached level four or the purple status. These numbers are updated every Thursday at 2:30 p.m.”
“As you raise the level, there’s additional guidance required recommended for the public. With level one, it just has to do with following current health orders, and there’s an advisory that there’s active exposure and spread. So daily health symptoms and self evaluation, staying at home maintaining distance wearing face coverings.
With level two and level three, the guidance builds. With our current level, it’s recommended that we decrease in-person interactions with others, consider necessary travel only, and limit attending gatherings of any number. That also builds on the previous guidance, so you’re supposed to follow level one, two and three.”
Ms. Smith then referred to seven critical indicators used for determining the seriousness of the COVID impact in the county. “Last Thursday,” she said, “…we triggered four of the seven indicators. We triggered indicator one – new cases per capita; indicator three – non-congregate cases met; indicator four – emergency department visits; and indicator five – outpatient visits. So I think it was in the next slide.
This is the data that we have available at the health department. From Thursday to Saturday, our new cases per capita have increased pretty significantly. Right now, we’re 7.5 times the CDC definition for high incidence, which is 100 new cases per capita, per 100,000 residents in Williams County, so that shows an increased risk of community spread.
We’ve also continued to trigger indicator three (non-congregate cases), indicator four (emergency department visits), and indicator five (outpatient visits). Now our outpatient visit trends continue to increase. It’s triggered by an increase in consecutive days. As we move closer to our current date in December, this trend continues to increase.”
“This week,” she continued, “…Williams County is number 57 out of 88 counties, and that just means that our incidence rate is ranked 57 out of 88. Last week, we were 60 out of 88 counties, but the week before we were 16 out of 88 counties. We have slowly moved down the list, but with our current incidence rate, increasing 92 cases since the last update for the past two weeks, it’s expected that we will probably rise on this list once again.
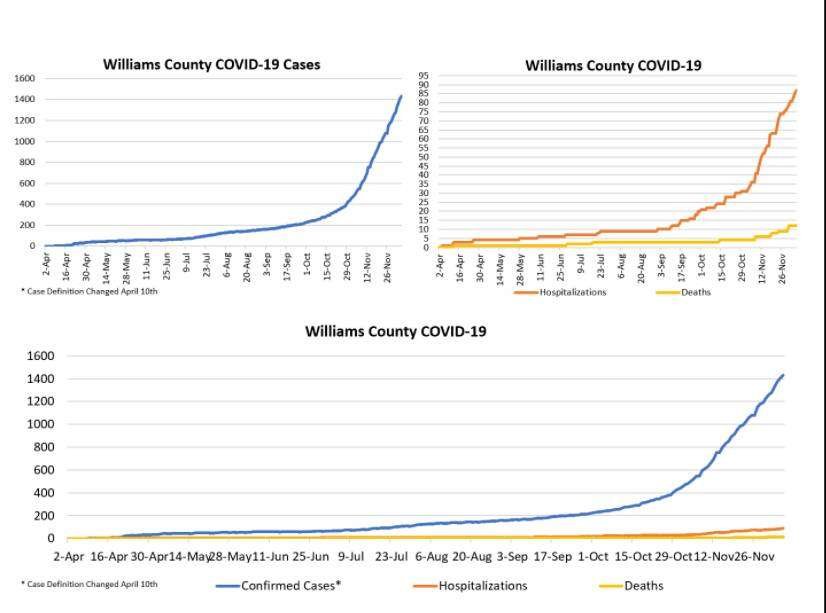
As of yesterday at 2 p.m., we have 1,433 cases. We have had 87 hospitalizations and 12 deaths in our county, and those are cumulative numbers. Just over the weekend, we had 58 new cases. We’ve had 440 new cases over the past 14 days, 24 hospitalizations, and 4 deaths. 63% of all Williams County cases were in the past month, and 59% and Williams County hospitalizations were in the past month as well. 67% of the deaths related to COVID-19 are also in the past month, so our rates have really increased over the past 30 days. Our rates have really increased since October for both cases, hospitalizations and deaths.
I also want to mention that hospitalizations and deaths typically lag behind, so the indicators may be a little bit slower. So as we see increasing trend in cases, that’s a pretty good indication that we will also see an increasing trend in hospitalizations and deaths in the coming weeks.”
Since the teleconference, the numbers have continued to spike.
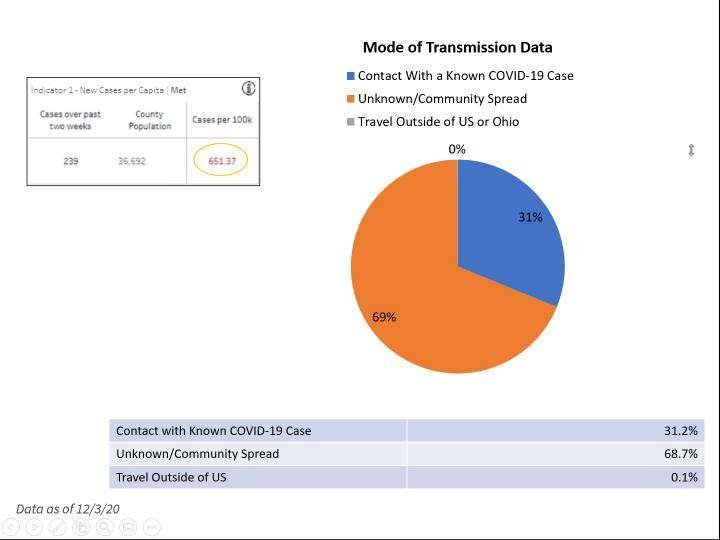
Data of December 3 showed Williams County with a 651.37 cases per 100,000 ratio over the two weeks prior. That number jumped to 744 cases per 100,000 by December 5, and as of December 10, Williams County is now at 992.04 cases per 100,000, with 364 new COVID cases over the past two weeks. Fulton County currently stands at 947.16 cases per 100,000, with Defiance County at 821.80 and Henry County at 840.55.
Again, the CDC definition for high incidence is 100 new cases per capita, per 100,000 residents of any given county. That being the case, Williams County is rapidly approaching the point where COVID cases exceed the CDC definition for high incidence by a factor of 10. In just three weeks, the COVID-19 case level per 100,000 residents has increased by 34% in Williams County. In Fulton County, the numbers have gone up by 37% in the same timeframe.
In discussing the modes of transmission, Smith said, “When we are doing contact tracing, one of our questions has to do with whether or not people have had contact with a known COVID-19 case…whether or not they know where they got COVID-19.
In the recent weeks, the unknown / community spread has increased pretty significantly.” As of December 3, contact tracing has determined that 68.7% of all new cases trace back to the unknown / community spread source category, with 31.2% having had contact with a known COVID-19 case, and 0.1% being traced to travel outside of the country.
Chad Tinkel said that from April through October, CHWC admitted 25 inpatients. “In the month of November,” he added, “…we admitted over 50 COVID inpatients…more than double in that 30 day period compared to the previous six months. On November 22, we hit our high of 16 COVID inpatients at one time.

For the last week, we’ve averaged about 10 COVID inpatients. We have concerns on what the impact of Thanksgiving will be. We saw a jump, a surge about 10 days after Halloween. We’re curious what we’ll see this coming week from the impact of Thanksgiving.” Speaking on load balancing efforts and staffing issues, Tinkel said, “We have converted our ICU and CCU units into COVID units. It has 16 beds.
We have moved our clean ICU, TCU, and med-surg patients to one area…that’s the ambulatory surgery area, and we’ve done this due to the limited staffing resources that we have. We have limited the number of admissions to out Montpelier inpatient due to staffing needs on the COVID unit, and we have limited inpatient elective procedures due to physical space limitations.”
“So continuing on with those resource limitations,” Tinkel added, “…our main limitation right now is staffing. We’ve had as many as 35 staff out related to positive tests, waiting on tests or contact tracing. We currently are with 20 staff that are out related to COVID. We are asking RNs that are willing to pick up shifts that do not normally work at the hospital, that may work at other medical facilities, or may have retired to consider coming back to help us out.
If they are interested, we ask that they contact the hospital’s HR Department so that we may utilize them to help with our limited resources of staffing. I mentioned the physical space limitations before, and the concerns with another surge in COVID patients. Our supplies from PPE: we are mainly doing fine in all the categories. There are certain unique items like medium sized gloves or gowns that we are having to go, if you will, to the secondary market to get those items.”
“One update on the current status of elective procedures and clinics,” Tinkel said in conclusion. “Both of these areas we are monitoring, and will scale back on an as-needed basis related to again the resources of staffing and physical space availability. The last item I want to talk about is our new visitor policy that we’ve had to reinstate on November 13.
This policy restricts visitation but allows some flexibility so that parents, guardians, pediatric patients may come in. Caregivers of dependent adults may come in. A support person for oncology patients, and one visitor per OB patient in labor; these are all the exceptions to our visitor policies.”
Sally Taylor provided an update on testing. “We continue to provide COVID-19 testing to the community. We’re able to provide the PCR and the point of care testing. The turnaround time for the PCR is greater than three days now due to limited resources at this point.
It’s important to note that within our facilities, it’s important that the patient sees a provider first, and then the provider will determine whether the testing is applicable. If there is a testing order from an outside agency, our lab locations are able to accept the PCR test, but we do not have an option for the point of care testing.
We also wanted to remind our patients that we’re here to care for them whether it’s for COVID, or other health care concerns. We don’t want patients to delay seeking care for any health condition. It’s important to keep your routine appointments to avoid worsening conditions or complications. Our offices are following safety precautions to keep our patients, providers and co-workers safe.

These include our enhanced cleaning procedures, social distancing measures, hand washing, and universal masking, and if needed, we are continuing to provide the opportunity for virtual or phone visits. Those are available for anyone who wants to seek care in the comfort of their home. We have been working with or collaborating with CHWC in referring patients for the antibody treatment, and that process has gone quite smoothly.
And in addition, we also have plans in place to ensure that we have adequate staffing and providers to care for the community like other health care organizations. We’ve experienced some staffing challenges with co-workers and providers who’ve been unable to work due to illness. Just to point out that the majority of those cases have been from community exposure and not exposure within the office.
We are proud of the…teamwork our coworkers have displayed throughout this pandemic, and we need the community’s help. The best way to show the support is to follow the guidelines: wear a mask, wash your hands, practice social distancing. The last thing I wanted to mention was we also continue to have our no visitor policy in place, with just a few exceptions.
So if we have a pediatric patient, a parent is allowed with the patient. If there’s an OB, then someone’s allowed to come in with the OB patient, or if you have a wheelchair or seeking infusion services.”

Dr. Park began with “I just want to give you a brief update of where we are in the nursing homes first, and then I’ll have a few coroner items to mention. I’m electing not to give the names of the nursing homes because I don’t have permission, but at this point there are four skilled facilities in the county that take in residents, and one of those facilities has a census of 97, and currently has 38 residents with COVID.
Pending more testing today, we have one facility with 66 residents, with one resident with COVID. We have another facility with 49 residents with 18, plus two more today equal to 20 active COVID cases. And we have a fourth with 20 positive cases out of 60 residents. The range of percentages of positive COVID are 1% in one facility, upwards to 63% of the residents of one facility either have COVID or had it.”

“The number of deaths is still fairly low,” Park continued, “…which is the good news if there’s some good news I have for you today. We’ve only had about three deaths, I believe from the nursing homes. A couple of those were residents that had been transferred from a Defiance facility.
We are treating a standard regimen using supplemental therapies including vitamin C, vitamin D and zinc.
Whether that has a factor and the outcomes, we’re not exactly sure. But we are at least pleased that the number of deaths has been low. We have a couple of residents that have been transferred to Bryan hospital and are currently there.
We have a couple that have been transferred to city hospitals with more severe symptoms. But for the majority of the residents that have tested positive, a fair number of those have been asymptomatic. A few of them have had symptoms such as just runny nose and loss of taste or smell. We are watching them in all facilities, doing respiratory assessments for low oxygen and hypoxia, and when they need regimens for hypoxia, are placed on oxygen and are transferred out, depending on family’s wishes.
I would say that the dedicated staff need to be thanked at the nursing facilities, because they’re risking their own health and lives in taking care of these residents. I want to thank them for that. There have been a fair number of positives, and we’ve had quite a few staff members at several the facilities that have come back before they’re in the quarantine and worked in the COVID unit with COVID themselves, so we’re very appreciative of those people.”
“From a coroner standpoint,” Park said in conclusion, “…the number of COVID deaths is more accurately depicted by Victoria’s numbers from the county; because it is a natural death when someone dies from pandemic COVID, so my data is not necessarily the data for the county.

I would tell you that I have 52 coroner’s cases this year, and last year, I had only approximately 40 cases. So the number of cases of coroner’s death has increased significantly. That trend that has to do some with an increased number of natural deaths of individuals who don’t seek medical help, and a fair number of increased drug overdose deaths.
Some of those are still pending toxicology, but the trend is for increased number of deaths statewide. The increased number of suicides and toxicologic deaths statewide, I spoke with multiple other coroners concerning this, and it does seem to be consistent straight across the state.”
In wrapping up the teleconference, Watkins said, “I think one of the important thing hopefully people take away today is that we all have a role to play in stopping the spread of COVID-19, to protect each other by wearing a mask, frequent hand washing, practicing social distancing so we can return to a strong economy.
Both the hospital and health department are participating and giving input on regular calls regarding vaccines that we are now starting to see on the horizon fairly soon. We hope to have additional information about that. As we receive that, we will get that out to the public so that everyone is aware of what’s going on with that.

So again, I just want to reiterate, there is no question that mask wearing, frequent hand washing and practicing social distancing work. We all want the same thing: a return to our healthy community. I strongly believe we can get there if we as individuals do our part.” On another note, there is some confusion in the public as to the purpose of the contact tracing process.
There are also some who see the call from a contact tracer as an infringement upon their personal liberties. “The purpose of the contact tracing call,” Mr. Watkins explained, “…is that when we have a person that has tested positive, we’re asking questions to determine if they were in contact with individuals for 15 minutes or greater, within six feet.
What the purpose of that is, is that those individuals we know have been exposed at that point…they have been exposed to an individual with the virus. So the purpose of the contact tracing is to find out who those individuals are, because those individuals may not realize that they were in contact with someone that did have COVID-19.
They could therefore unknowingly be in the community, in settings, and exposing others. So what we are trying to do is corral the virus and prevent it from taking that opportunity to infect others, and that’s one of the difficult things I think about this virus is that it is very good about moving from person to person.

Therefore it is very easily spread in the community, so if we can rope it in so to speak, we can stop that transmission. So if we can have those folks help us and help everyone else in the community, we will start to see the amount of COVID in the community go down.”
Tim can be reached at tim@thevillagereporter.com